
From the 1Department of Health Sciences, Lund University, Lund, 2Department of Neurology and Rehabilitation Medicine, Skåne University Hospital, Lund, 3Department of Health Sciences, Luleå University of Technology, Luleå, Sweden, and 4School of Health and Exercise Sciences, University of British Columbia, Okanagan Campus, Kelowna BC, Canada
Objectives: To assess the presence of depressive symptoms among older adults with long-term spinal cord injury and investigate the association with sociodemographic and injury characteristics; and to determine how potentially modifiable factors, i.e. secondary health conditions, sense of coherence, coping strategies and leisure-time physical activity, are associated with depressive symptoms.
Design: Cross-sectional study.
Subjects: A total of 122 individuals (70% men, injury levels C1–L5, American Spinal Injury Association Impairment Scale A–D), mean age 63 years, mean time since injury 24 years.
Methods: Data from the Swedish Aging with Spinal Cord Injury Study, collected using the Geriatric Depression Scale-15, the 13-item Sense of Coherence Scale, the Spinal Cord Lesion-related Coping Strategies Questionnaire and the Physical Activity Recall Assessment for people with Spinal Cord Injury. Associations were analysed using multivariable linear regression.
Results: A total of 29% reported clinically relevant depressive symptoms and 5% reported probable depression. Sense of coherence, the coping strategy Acceptance, neuropathic pain and leisure-time physical activity explained 53% of the variance in depressive symptoms.
Conclusion: Older adults with long-term spinal cord injury report a low presence of probable depression. Mental health may be supported through rehabilitation that strengthens the ability to understand and confront life stressors, promotes acceptance of the injury, provides pain management and encourages participation in leisure-time physical activity.
Key words: adaptation, psychological; ageing; depression; exercise; rehabilitation; sense of coherence; spinal cord injury.
Accepted May 30, 2017; Epub ahead of print Aug 1, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Sophie Jörgensen, Department of Health Sciences, Rehabilitation Medicine Research Group, PO Box 157, Lund University, SE-221 00 Lund, Sweden. E-mail: sophie.jorgensen@med.lu.se
Many people with long-term spinal cord injury (SCI) now reach older age; therefore knowledge of factors associated with their healthy ageing is needed. According to the World Health Organization (WHO) (1), healthy ageing refers to the process of developing and maintaining the functional ability to be and to do what is perceived as valuable, which enables well-being in older age. This ability is determined by the interaction between a person’s physical and mental capacities and their environment. As maintained mental health is a key element of healthy ageing, the psychological aspects of living with long-term SCI into older age deserve more attention.
Depression is one of the most common psychological conditions among older adults in the general population (2) and the risk of developing depression has been found to increase after SCI (3, 4). It has been suggested that depressive symptoms after SCI are more closely related to psychological factors and behaviours than to sociodemographic factors, such as age and gender, and injury characteristics, such as level and severity of injury (5–7). However, very few studies have specifically assessed older adults with long-term SCI. In the general population, depression in older age is associated with increased disability and mortality (8). Consequently, depressive symptoms might have greater consequences for older adults with long-term SCI compared with younger adults (4) and the non-injured ageing population (9). To support mental health among older adults with long-term injury, there is a need for increased knowledge of depressive symptoms and associated factors.
Previous SCI research indicates a relationship between depressive symptoms and potentially modifiable factors, such as secondary health conditions (SHCs) (e.g. pain, bowel and bladder dysfunction) (10, 11) and personal factors (e.g. sense of coherence (SOC) and coping strategies) (3, 12–14). SOC (15) refers to a salutogenic concept inferring that the way people view their lives determines their ability to preserve good health despite external hardship. Coping comprises varying cognitive and behavioural strategies used to handle demands perceived as burdensome (16). Moreover, depressive symptoms are related to health behaviours. Studies have shown beneficial effects of leisure-time physical activity (LTPA); i.e. physical activity performed during free time, on depressive symptoms in the general population (17), in older adults (1) and after SCI (18, 19). However, SCI research includes mostly younger and middle-aged persons and it is unclear whether the relationships between depressive symptoms and these modifiable factors also hold true among older adults with long-term injury.
Taken together, several aspects of mental health among older adults with long-term SCI are largely unknown. Thus, the aims of this study are: (i) to assess the presence of depressive symptoms among older adults with long-term SCI and to investigate the association with sociodemographic factors and injury characteristics; and (ii) to determine how potentially modifiable factors, i.e. SHCs, SOC, coping strategies and LTPA, are associated with depressive symptoms.
We hypothesize that potentially modifiable factors are stronger explanatory factors for depressive symptoms than sociodemographic factors and injury characteristics, and that SOC, coping strategies and LTPA are each independently associated with depressive symptoms among older adults with long-term SCI.
This study is part of the Swedish Aging with Spinal Cord Injury Study (SASCIS) (for details, see Jörgensen et al. (20)). SASCIS is a population-based, longitudinal cohort survey study assessing individuals 50 years or older and at least 10 years after SCI. The SASCIS aims to contribute to the knowledge base of factors associated with healthy ageing in individuals with long-term SCI.
The participants were community-dwelling and recruited through databases available at the SCI Unit at Skåne University Hospital in Lund, Sweden. Each year, the SCI Unit admits 35–55 individuals with SCI for primary rehabilitation and serves a catchment area of approximately 1.8 million people. At the time of recruitment (year 2011), 184 individuals met the inclusion criteria of the SASCIS (i.e. 50 years or older and at least 10 years after traumatic SCI or non-progressive, acquired non-traumatic SCI) and the final study sample comprised 87 men and 36 women with a mean age of 63 years (range 50–89 years) (20). According to the American Spinal Injury Association (ASIA) Impairment Scale (AIS) (21), 3 groups of SCI severity were formed: (i) tetraplegia AIS A-C (n = 22; 15 AIS A, 4 AIS B and 3 AIS C); (ii) paraplegia AIS A-C (n = 41; 23 AIS A, 8 AIS B and 10 AIS C); and (3) all AIS D (n = 60) (20).
Before enrolment, all participants were given written and oral information about the study, and provided their written informed consent to participate. The principles of the Declaration of Helsinki for research on humans were followed and the SASCIS was approved by the Regional Ethical Review Board in Lund, Sweden (number 2010/692).
Sociodemographics and injury characteristics. Data collection was performed via interviews in the participants’ homes (n = 122) or in another location (n = 1). Data on sociodemographics (gender, age, marital status, vocational situation and residential location) and injury characteristics (age at injury, time since injury, cause of injury, level and severity of injury and use of a mobility device outdoors) were obtained from a study-specific questionnaire and the participants’ medical records.
Depressive symptoms. To assess the presence of depressive symptoms, the 15-item Geriatric Depression Scale (GDS-15) (22) was used. The scale consists of 15 questions with dichotomous responses (yes/no), such as “Do you feel that your life is empty?” (22). The participants were asked to answer the questions in reference to how they have felt over the past week (22). The total score ranges from 0 to 15, where greater scores indicate more symptoms of depression. A score of 5 or more suggests clinically relevant depressive symptoms and a score of 10 or more indicates probable depression (23). The GDS-15 has demonstrated evidence of reliability, validity and ability to discriminate between depressed and non-depressed older adults (22, 23). The Cronbach’s alpha in the present study was 0.77. The GDS-15 was chosen as it does not contain questions related to somatic symptoms of depression (e.g. sleep disorders and pain), which may overlap with symptoms related to SCI and ageing.
Secondary health conditions (SHCs). Data on bowel-related and bladder-related problems (i.e. bowel and urinary incontinence, constipation, diarrhoea, bowel irregularity, haemorrhoids, flatulence, urinary urgency and frequent urinary tract infections), nociceptive and neuropathic pain, and spasticity were obtained from a study-specific questionnaire. SHCs were recorded as present if the participants reported them to recur during the past year. For pain, the participants were asked to rate the greatest pain intensity experienced in everyday life on a standard visual analogue scale for Pain (0–100 mm, ranging from “no pain” to “worst imaginable pain”). Pain intensity was classified as mild (5–44 mm), moderate (45–74 mm) or severe (75–100 mm) (24), and dichotomized into no/mild pain vs moderate/severe pain.
Sense of coherence (SOC). To assess SOC (15), the 13-item SOC Scale (SOC-13) was used. The participants graded the items on a 7-point Likert scale, ranging from agreement to disagreement with statements related to the SOC dimensions (i.e. comprehensibility, manageability and meaningfulness). Comprehensibility refers to the ability to understand the surrounding environment, manageability is the capacity to manage a given situation on one’s own or with the help of others, and meaningfulness represents the ability to find the situation meaningful (25). The total sum score ranges from 13 to 91 and higher scores indicate a stronger SOC. The SOC-13 has demonstrated satisfactory internal consistency and validity (25). The Cronbach’s alpha in the present study was 0.84.
Coping strategies. To assess coping strategies, the Spinal Cord Lesion-related Coping Strategies Questionnaire (SCL CSQ) (26) was used. The questionnaire consists of 3 subscales labelled: (i) Acceptance (revaluation of life values); (ii) Fighting spirit (efforts to behave independently); and (iii) Social reliance (a tendency towards dependent behaviour) (26). The participants rated the 12 items on a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree), in reference to how they felt at the time of the interview. Scores are presented as the mean of the ratings in each subscale, with higher scores indicating greater use of the corresponding coping strategy (27). The scale has demonstrated evidence of validity and internal consistency in persons with SCI (26). The Cronbach’s alpha in the present study was 0.74 for the Acceptance subscale, 0.39 for the Fighting spirit subscale and 0.78 for the Social reliance subscale; as the Fighting spirit subscale did not reach an acceptable internal consistency level it was not included in the analysis.
Leisure-time physical activity (LTPA). To assess LTPA, the Physical Activity Recall Assessment for people with Spinal Cord Injury (PARA-SCI) (28) was used. The PARA-SCI was designed to capture the intensity, duration, type and frequency of all physical activities performed during the past 3 days, including LTPA (e.g. sports, going for a walk/wheel) and activities of daily living (e.g. dressing, grocery shopping, transfers). For the present study, the mean number of minutes per day of LTPA of all intensities and types was used. The PARA-SCI has demonstrated evidence of construct validity and the test-retest reliability is comparable to other self-report measures of physical activity (28). A detailed description of LTPA participation and associated factors within the SASCIS study sample has been presented elsewhere (29).
Data management. From the original SASCIS study population (n = 123) (20), 122 participants had completed the GDS-15 and were included in this study. To generate complete data for each participant, imputation was used for missing data. For the GDS-15, 5 participants had missing data on less than 4 items; the missing values were replaced by the mean value of the reported item scores for the respective participant (30). For the SOC-13, 3 participants had missing data on 1 item; the missing value was replaced by the mean value of the reported item scores for the respective participant. Two participants were excluded due to extensive missing data on the SOC-13. For the SCL CSQ, the developers recommend calculation of the sum score for each subscale if less than half of the items are missing; this applied to 7 participants. For the PARA-SCI data, 119 participants had completed the assessment and we identified 2 outliers (greater than the mean ± 3 standard deviations (SD)) that were reduced to 1 unit less than the next lowest value in the distribution (31).
Statistical analysis. Descriptive statistics are presented for sociodemographics, injury characteristics, depressive symptoms, SHCs, SOC, coping strategies and LTPA. To further describe depressive symptoms, differences between groups (e.g. men and women, groups based on level and severity of injury) in the number of depressive symptoms and percentages of participants scoring above the cut-off for clinically relevant depressive symptoms (GDS-15 ≥ 5) were assessed with the Kruskal–Wallis test, the Mann–Whitney U test, or the χ2 test, as appropriate. For the Kruskal–Wallis test, post-hoc pairwise comparisons with Bonferroni adjusted p-values were performed (32). Effect sizes (r) and odds ratios for the significant differences were calculated (32). Bi-variable correlations between the number of depressive symptoms and age, time since injury and age at injury were assessed with the Spearman’s rank correlation coefficient.
To investigate associations between depressive symptoms (dependent variable) and sociodemographics and injury characteristics (independent variables), a multivariable linear regression analysis was performed. To identify the sociodemographic and injury-related variables with the strongest associations with depressive symptoms, a backward elimination procedure was applied, and variables that did not make a statistically significant contribution to explaining the variance in depressive symptoms were sequentially removed (32) until all independent variables in the model had a p-value less than 0.10. The model exhibited no residual outliers or influential cases, no multicollinearity and no heteroscedasticity.
To investigate associations between depressive symptoms (dependent variable) and the potentially modifiable factors (independent variables) a second multivariable linear regression analysis was performed using a backward elimination procedure until all independent variables in the model had a p-value less than 0.10. Finally, we investigated the variance explained by sociodemographics, injury characteristics and the potentially modifiable factors together. The independent variables that remained in the first regression model (i.e. vocational situation, cause of injury, level and severity of injury and use of mobility device outdoors) were entered into a multivariable linear regression model together with the independent variables from the second multivariable model (i.e. neuropathic pain, SOC, the coping strategy Acceptance and LTPA) (backward elimination). This procedure in 3 steps was chosen because inclusion of all possible independent variables in 1 model would have resulted in overfitting (32) the multivariable regression model. The models exhibited no residual outliers, no influential cases, no multicollinearity, no heteroscedasticity and the residuals were normally distributed.
All analyses were conducted using SPSS v. 22 software for Windows (IBM Corporation, Armonk, NY, USA). p-values less than 0.05 denote statistical significance and exact significance levels are reported.
Data on the participants’ sociodemographic and injury characteristics are presented in Table I. Their mean age was 63 years, mean time since injury 24 years and the majority (70%) were men. Just over half of the participants (53%) were living in a relationship and approximately one-third (35%) were working full-time or part-time. A large majority (73%) used a manual or powered wheelchair/scooter as the primary mode of mobility for longer distances outdoors.
Table I. Sociodemographics and injury characteristics of older adults with long-term spinal cord injury (n = 122)
For the total sample, the mean number of depressive symptoms was 3.4 (± SD) 2.9, min–max 0–12, median 3.0, Q1–Q3 1.0–5.0). In Table II, descriptive statistics for the number of depressive symptoms (GDS-15 scores) in relation to sociodemographics and injury characteristics are presented. Participants who had a partner and/or were working reported significantly fewer depressive symptoms than those who were single and/or unemployed (p = 0.015, r = –0.22 and p < 0.001, r = –0.32, respectively). There were no significant associations between the number of depressive symptoms and chronological age, time since injury or age at injury. A total of 17 participants (14%) used antidepressants; they did not differ significantly from participants without antidepressants regarding the number of depressive symptoms.
Table II. Depressive symptoms (assessed with the 15-item Geriatric Depression Scale; GDS-15) in relation to sociodemographics and injury characteristics among older adults with long-term spinal cord injury (n=122)
Less than one-third of the participants (n = 35, 29%) scored above the cut-off for clinically relevant depressive symptoms (GDS-15 total score ≥ 5) and 6 participants (5%) reported ≥ 10 depressive symptoms, indicating probable depression. Participants who were unemployed were more likely to report clinically relevant depressive symptoms compared with those who were working full-time or part-time (p = 0.011, odds ratio (OR) 3.6). There were no other significant differences regarding sociodemographics, injury characteristics or use of antidepressants between participants scoring above the cut-off for clinically relevant depressive symptoms compared with those scoring below.
In Table III, the multivariable linear regression analysis investigating associations between the number of depressive symptoms and sociodemographics and injury characteristics is presented. The independent variables explained 13% of the variance in depressive symptoms. Non-traumatic injury, working full-time or part-time and a tetraplegia or paraplegia AIS A-C injury (compared with an AIS D injury) were significantly associated with fewer symptoms of depression. The use of a powered wheelchair/scooter (compared with use of walking devices/no mobility device) was significantly associated with more symptoms of depression.
Table III. Multivariable linear regression model showing the associations between depressive symptoms (assessed with the 15-item Geriatric Depression Scale; GDS-15) as dependent variable and sociodemographics and injury characteristics among older adults with long-term spinal cord injury (n = 122)
In total, 32% and 43%, respectively, reported bowel- and bladder-related problems. Spasticity was reported by 43%, moderate/severe nociceptive pain was reported by 40% and 50% experienced moderate/severe neuropathic pain.
In Table IV, descriptive statistics for SOC, coping strategies and LTPA are presented. SOC scores ranged from 37 to 91, with a mean total score of 71 (median 73). The participants used the coping strategies Acceptance and Social reliance to a similar degree, with mean total scores of 2.7 and 2.8, respectively. There was a large variation in daily LTPA among the participants and they reported, a mean of, 35 min of LTPA per day (median 15 min per day).
Table IV. Sense of coherence (SOC), coping strategies and leisure-time physical activity (LTPA) among older adults with long-term spinal cord injury
The multivariable linear regression analysis investigating the associations between the number of depressive symptoms and SHCs, SOC, coping strategies and LTPA is presented in Table V. The independent variables explained 53% of the variance in the number of depressive symptoms. Moderate/severe neuropathic pain was significantly associated with more depressive symptoms. Conversely, a stronger SOC, greater use of the coping strategy Acceptance and more minutes per day of LTPA were significantly associated with fewer symptoms of depression, with SOC being the strongest contributor to the model. When combining this model with the sociodemographic and injury-related variables from Table III, the resulting final multivariable model was identical to the model presented in Table V.
Table V. Multivariable linear regression model showing the associations between depressive symptoms (assessed with the 15-item Geriatric Depression Scale; GDS-15) as dependent variable and secondary health conditions, sense of coherence (SOC), coping strategies and leisure-time physical activity (LTPA), among older adults with long-term spinal cord injury (n = 118)
To the best of our knowledge, this is the first study to investigate depressive symptoms and associated factors in a sample of older adults with long-term SCI in Sweden. Overall, the participants reported few depressive symptoms. Approximately one-third had clinically relevant depressive symptoms, but only 5% had signs of probable depression. Our hypotheses were supported as sociodemographics and injury characteristics explained minimal variance in the number of depressive symptoms, whereas the potentially modifiable factors explained more than half of the variance. SOC was the strongest explanatory factor for depressive symptoms, although significant associations were also found for neuropathic pain, the coping strategy Acceptance and LTPA. As maintained mental health is a key element to enable well-being in older age, this study indicates that older adults with long-term SCI have some characteristics and strategies that may support healthy ageing.
The findings of this study indicate that clinically relevant depressive symptoms seem to be more prevalent among older adults with long-term SCI compared with the non-injured older population. A review of depression in late life noted that 8–16% of older people report such symptoms (8). A recent Swedish study of older adults in the general population showed that 9.8% reported depressive symptoms (33). Conversely, our participants demonstrated a lower rate of probable depression than in previous studies of people with SCI (i.e. 9–25%) (3, 4, 6), including individuals with long-term injury, and comparable to the prevalence of major depression in non-disabled older people (i.e. 1–5%) (8, 34). As depressive symptoms can decrease over time following SCI (3), and all of the participants were at least 10 years post-injury, the demographics of our sample may, at least in part, explain the discrepancy. Another explanation may be that psychological support within healthcare and social service systems differ between Sweden and other countries where SCI and depression data have been reported. In addition, the use of different assessment tools can lead to varying results regarding the number of depressive symptoms, which attests for a need to reach consensus on how to assess depressive symptoms among individuals with SCI.
The low rate of probable depression indicates that older adults with long-term SCI in Sweden are well adjusted to their altered life situation. Thus, one can assume that the SCI-specific lifelong follow-up programme provided by Swedish healthcare is a valuable source of support for this group. However, the present study indicates that clinically relevant depressive symptoms are not uncommon among older adults with long-term SCI. It is known that, once developed, depressive symptoms in people with SCI can be persistent (6) and that there is under-recognition of such symptoms in the general ageing population (4). Consequently, a routine evaluation of depressive symptoms among older adults with long-term SCI would identify those at risk of developing probable depression, and thereby enable early interventions.
In the multivariable analysis, employment was associated with fewer depressive symptoms, which corroborates results from previous studies of individuals with SCI (10, 35). We have reported a positive relationship between employment and life satisfaction in the SASCIS study sample (36). More in-depth analyses are needed to understand how the complexity of factors associated with employment, such as financial security, meaningful and productive activities and social context, may contribute to well-being in this population.
A less severe SCI (i.e. AIS D) was associated with more symptoms of depression than a more severe injury (i.e. AIS A-C). This might not be expected, but similar results were, in fact, described in a longitudinal study (n = 801, mean time since SCI 15 years) where participants with non-ambulatory injuries had lower odds of depression than those who were ambulatory (6). Research suggests that individuals with less severe SCI can perceive a lack of understanding for their disability (37) and that pain is more common in individuals with AIS D injuries (38), which may influence their mood. In light of these findings, it may seem somewhat contradictory that the use of a powered wheelchair/scooter was significantly associated with more symptoms of depression in our sample. However, individuals with SCI can perceive the wheelchair as the most limiting factor for their perceived participation (39), and participation restrictions are associated with more symptoms of depression (5). Further studies are needed to understand the association between depressive symptoms, mobility and use of powered mobility devices among older adults with long-term SCI, and to what extent injury severity interacts with these factors.
Taken together, this multivariable analysis revealed some significant associations between depressive symptoms and sociodemographics and injury characteristics. However, the amount of variance explained was small and none of these variables remained in the final model with the potentially modifiable factors. This is encouraging, as almost all of the investigated sociodemographics and injury characteristics are not modifiable by intervention.
Our hypotheses were supported as SHCs, SOC, coping strategies and LTPA together explained more than half of the variance in the number of depressive symptoms. Of these, SOC was the strongest contributing factor to the explained variance. This indicates that older adults with long-term SCI who have the ability to understand and handle external strains and to stay motivated when they occur are less likely to report depressive symptoms. The association between SOC and depressive symptoms has been reported in the general population (40) as well as among individuals with SCI (14). The relationship between a strong SOC and resilience, as well as a subjective experience of better physical health (40) may explain this finding. The association between the coping strategy Acceptance and fewer depressive symptoms has consistently been reported in individuals with SCI (14). Acceptance is different from resignation and comprises setting new priorities and thereby reducing the importance of the changes imposed by the injury (27). As such, it intuitively has a positive effect on mental health. The strong association between depressive symptoms and SOC and coping supports the contention that strengthening of psychological resources can reduce depressive symptoms after SCI (3).
The results of the present study show that the well-known relationship between physical activity and depressive symptoms (17, 18) holds true also for older adults with long-term SCI. Mechanisms potentially underlying this association are the positive effects of LTPA on self-efficacy, neurochemical mechanisms (e.g. alteration of neurotransmittors and neurogenesis) and social interaction (17). We have reported previously that the SASCIS participants do not reach a sufficient amount of LTPA to achieve fitness benefits (29). Whether increased participation in LTPA has a positive effect on their mental health is an interesting topic for future studies.
Surprisingly, neuropathic pain was the only SHC significantly associated with depressive symptoms. This indicates that rehabilitation professionals should be attentive to depressive symptoms among individuals seeking consultation for neuropathic pain. It may be that other SHCs, although considered an inconvenience, have become part of everyday life and those affected have found strategies to limit their impact. However, as we did not ask for the frequency, duration or perceived impact of recurring SHCs, we may not have identified participants truly restricted by these conditions.
Taken together, the potentially modifiable factors investigated in this study explained more than half of the variance in depressive symptoms. Thus, further studies should evaluate to what extent strengthening of psychological resources, pain management programmes and strategies to promote LTPA participation can reduce depressive symptoms among older adults with long-term SCI.
Several strengths of the SASCIS have previously been discussed, such as the representative study sample and the use of valid, reliable and internationally used assessment tools (20, 29, 36). A limitation is the cross-sectional study design that does not allow us to identify causal relationships. Regarding SHCs, the greatest pain intensity experienced in everyday life was registered, which could have led to an overestimation of pain intensity. Spasticity was not clinically examined, which should be taken into consideration when interpreting the results. LTPA was measured using a self-report assessment tool, which could be susceptible to recall-bias, although objectively measuring LTPA was not feasible given the large study sample and practical circumstances for data collection in a geographically dispersed study district.
Older adults with long-term SCI in Sweden generally report few depressive symptoms, a low presence of probable depression and a strong SOC. As depressive symptoms do occur, to identify those at risk of developing probable depression and thereby enable early interventions, we recommend routine evaluation of mental health in this population. The associations identified suggest that mental health among older adults with long-term SCI may be supported through rehabilitation programmes that strengthen the ability to understand and confront life stressors, promote acceptance of the injury, provide adequate pain management and encourage LTPA participation.
The authors wish to thank all participants. The authors are grateful to Lizette Norin, BSc, Department of Health Sciences, Lund University, for her involvement in the data collection, and to Susann Ullén, PhD, Clinical Studies Sweden Forum South, Skåne University Hospital, for valuable statistical advice. This study was carried out within the framework of the Swedish Aging with Spinal Cord Injury Study (SASCIS), financed by research grants from the Swedish Research Council, the Norrbacka-Eugenia Foundation, the Promobilia Foundation, the Research Fund of Neuro Sweden, the Swedish Association for Survivors of Accident and Injury (RTP), Gun och Bertil Stohne’s Foundation, the Ribbingska Foundation in Lund, and the Gustaf V and Queen Victoria’s Freemason Foundation. Dr Jörgensen is the recipient of a PhD grant from the Norrbacka-Eugenia Foundation. The SASCIS was accomplished within the context of the Centre for Ageing and Supportive Environments (CASE), Lund University, financed by the Swedish Research Council for Health, Working Life and Welfare.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize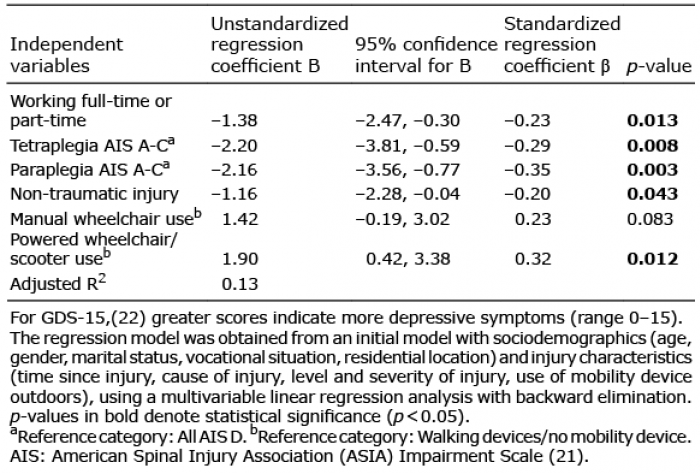 Click to show fullsize
Click to show fullsize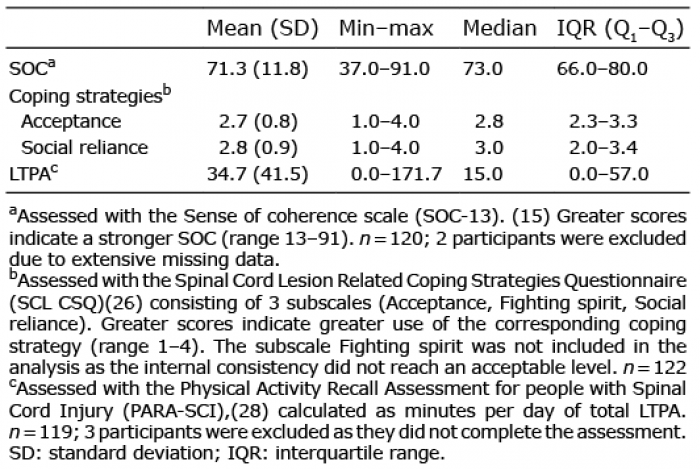 Click to show fullsize
Click to show fullsize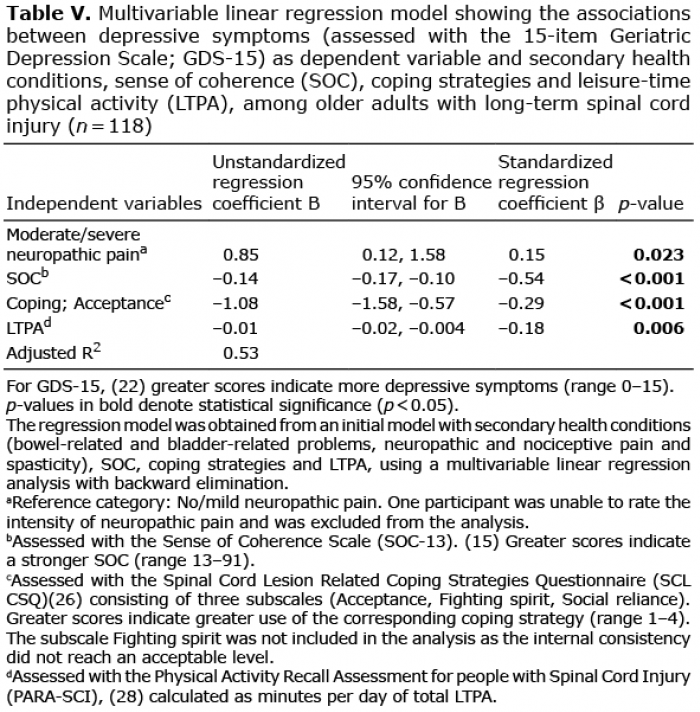 Click to show fullsize
Click to show fullsize